
Insulin resistance is an inability of tissues to "hear" the insulin signal properly, leading to poor blood glucose handling and other metabolic problems in processes that depend on insulin. In my interview with Aitor Calero, I made the statement that the main cause of insulin resistance is excess body fat. To be more precise, body fatness is the main modifiable cause*-- genetic makeup is another major factor that you're stuck with regardless of lifestyle. Diabetes is caused by insulin resistance plus the eventual failure of the insulin-secreting pancreatic beta cells. Some people become obese and insulin resistant, but their beta cells never fail, and therefore they do not become diabetic. This has a strong genetic component, as Gretchen mentioned in the comments. If you look at genetic loci associated with type 2 diabetes risk, most of them are in genes that regulate the pancreas, although the strongest obesity locus FTO is also a diabetes risk factor (0).
Regardless, there can be no question that body fatness is tightly associated with diabetes risk. For example, in the Health Professionals Follow-up study, among 52,000 men, body mass index (a rough estimate of fatness) predicted the risk of developing diabetes over five years (1). A BMI of 25 or more suggests overweight, and a BMI of 30 or more suggests obesity. The data are striking:

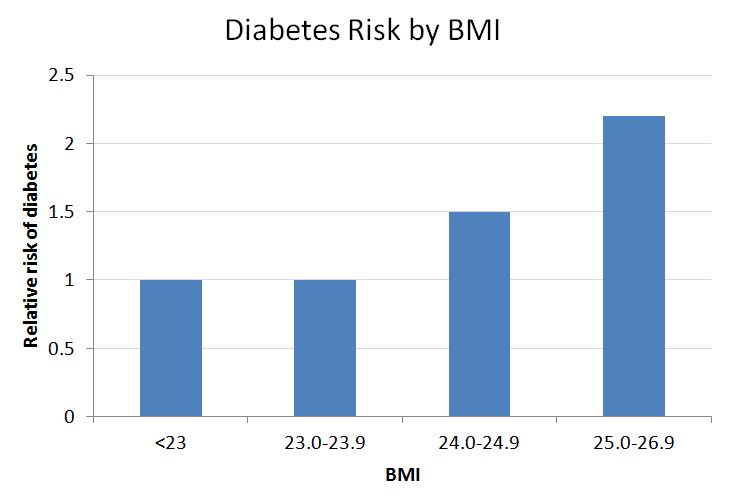
As I've explained in the past, multiple lines of evidence suggest that this is because excess body fat causes insulin resistance, which in turn increases the risk of developing diabetes* (1A, 1B).
I understand that this is frustrating to people who carry excess fat and have a hard time losing it. For many people, fat loss is a real challenge, and achieving true leanness is unlikely. If that's you, I have some good news. First of all, you can reduce your diabetes risk without losing a pound, by exercising regularly, eating a whole food diet, and managing sleep and stress effectively. Second, you can greatly reduce your diabetes risk by losing as little as 11 pounds (5 kg).
This was demonstrated by the striking results of the Diabetes Prevention Program study, involving 3,234 pre-diabetic volunteers (2). In this study, a combination of weight loss (via calorie-restricted low-fat diet) and exercise reduced the risk of developing diabetes by a full 58 percent over 2.8 years. A similar trial in Finland a year earlier produced a virtually identical result (3), and similar results have come from trials in India, Japan, and China (4, 5, 6). This kind of risk reduction is virtually unheard of in lifestyle modification trials, particularly considering the typical half-hearted adherence-- this shows that the intervention was striking directly at the heart of the problem. It's possible that weight loss via a different diet (e.g. Paleo) would have been even more effective, but we won't know for sure until it's tested.
A follow-up study tried to determine which aspect of the DPP intervention was most important for diabetes risk reduction (7). Here's what they found:
Weight loss was the dominant predictor of reduced diabetes incidence (hazard ratio per 5-kg weight loss 0.42 [95% CI 0.35-0.51]; P less than 0.0001). For every kilogram of weight loss, there was a 16% reduction in risk, adjusted for changes in diet and activity. Lower percent of calories from fat and increased physical activity predicted weight loss. Increased physical activity was important to help sustain weight loss. Among 495 participants not meeting the weight loss goal at year 1, those who achieved the physical activity goal had 44% lower diabetes incidence.There you have it, folks. We know how to prevent type 2 diabetes, and it's not magic. These simple steps will reduce your risk:
- If you're overweight, lose fat if you can, even as little as a few pounds
- Exercise regularly
- Eat a healthy diet
* I simplify for a general audience, but it's probably more complicated than this. Cellular energy overload causes insulin resistance, and this occurs when fat tissue expands to the point where it no longer efficiently traps fatty acids, exposing tissues throughout the body to excess energy. In addition, enlarged fat depots tend to become inflamed, and inflammation contributes to insulin resistance. So the causality is probably something like this: excess energy intake leads to excess fat mass, which leads to poor fatty acid trapping and inflammation in fat cells, which leads to cellular energy excess and inflammation in lean tissues, which leads to insulin resistance. Although the full story is more nuanced, it is nevertheless fair and accurate to distill this down to the statement that excess body fat causes insulin resistance and diabetes. This is true even though there is not a 1:1 correspondence between obesity and insulin resistance.
54 comments:
I once gave a talk on type 2 diabetes at the local hospital, and one thing that surprised me was how few of the people in the audience were significantly overweight.
There was one man with a "beer belly," typical of metabolic syndrome. But most of the people were middle-aged or elderly women, some what I would call "grandmotherly shaped," that is, not skinny (which isn't healthy in older people) but not really fat. Some were quite thin. Maybe they were misdiagnosed LADA.
Now this is annecdotal, and perhaps the participants were self-selected. Maybe the real fat ones were embarrassed to come.
But our beta cells wear out with age, just like the rest of us, and this also contributes to type 2.
The "classic" view of type 2 is that overstimulation caused by IR "burns out" the beta cells, but more recent analyses have suggested that this might not be correct.
BTW, I think I was a classic case of type 2, I was definitely overweight when Dx'd. I lost 20% of my body weight and now have a BMI in the normal range, but this had no effect on my blood glucose. Many patients say they were told that losing just 5 or 10 pounds might reverse their condition, and they found that weight loss had no effect.
I was in a clamp study at Joslin and they said my IR (after the weight loss) was "right in the middle of what we'd expect of someone with type 2," although less than they find with really obese people.
So in my case, obesity was most likely the main cause, although the disease has hit 4 members of my family. IOW, I 'm not trying to argue that I'm totally innocent. I'm arguing on behalf of the people who were normal weight and exercised and got type 2 anyway.
If both your parents have type 2, your risk is extremely high, and many such people get the disease in their 30s. There's evidence that nondiabetic relatives of people with type 2 have defects in their mitochondria.
However, I agree that the risk is much greater in overweight people. But there are probably more people at the extremes of the bell curve than we realize today.
Cellular energy overload causes insulin resistance
I dislike that line of thinking because it doesnt make logical sense. Cells are always swimming in a sea of excess energy, regardless of the adiposity of the host.
What scale are you using to define "energy excess"?
Cells always see abundance of energy because serum FFA and serum glucose never have an instantaneous value of zero. roughly speaking.
In this study they fed a high-fat diet but clamped fat mass to prove that it is the increase in fat mass that wrecks insulin homoeostasis not a high-fat diet....
However
One also needs to consider this study which destroys the lipotoxicity theory. These studies combined suggest that it is not the presence of increased adiposity itself which is the cause of insulin resistance but rather there is something else causing it that goes hand in hand with increased fat mass.
Thanks for posting this. I'm at high risk of Type II (morbidly obese, and my dad died at age 53 from diabetic complications after having his first heart attack at 38 - one year older than I am now), and it's always good to get a reminder.
"These studies combined suggest that it is not the presence of increased adiposity itself which is the cause of insulin resistance but rather there is something else causing it that goes hand in hand with increased fat mass."
Kindke, could it be the 'mild', chronic intoxication with lipopolysaccharides produced in the upper intestine by gram negative critters that thrive on evolutionary unprecedented loads of dense, 'acellular' carbohydrate sources (aka grains)?
This hypothesis by Ian Spreadbury (if true) would explain a lot:
http://www.dovepress.com/articles.php?article_id=10339
(download button under the abstract).
Melchior,
Or it could actually be the critters on the meat we eat, that get through the gut wall:
http://www.youtube.com/watch?v=p_uy4kfQDkA&feature=plcp
Has anyone ever considered/or stopped to question the 'normal range' for BMI might be a little HIGH to show a significant reversal. So, when some people fail at seeing a reversal in their insulin resistance, when they meet the 'normal range', if they just lost a little more they might be surprised. I suppose this idea is politically incorrect, because it might look like adults should actually look a little more like the celebrity ideal. Alternatively,
"Having a BMI of 24-24.9, which isn't even considered overweight, was associated with a 50 percent higher risk of diabetes, and going just over the cusp of overweight yielded a 120 percent increase in risk. Therefore at nearly all levels of BMI, higher BMI strongly predicted the risk of developing diabetes. This has been repeatedly confirmed."
So - does this mean that EVERY athlete in the world who has ahigh BMI do to their increased muscle mass is in severe danger of developing Type 2 diabetes??
This doesn't make much sense.
Charles Grashow said...
"So - does this mean that EVERY athlete in the world who has ahigh BMI do to their increased muscle mass is in severe danger of developing Type 2 diabetes??"
No, because the above data are from the Health Professionals Follow-up study, not the Athletes Follow-up study. In athletes, BMI doesn't correlate with fat mass.
I have read the DPPT research. You are missing in important point. The DPPT considered someone diabetic if they tested over 200 mg/dl at 2 hours on the oral glucose tolerance test and "not diabetic" if they tested at 199 mg/dl at 2 hours on the test.
There is no question that diet and exercise can make a difference of 10 mg/dl in blood sugar response, and over a very brief period (less than 3 years) that will make it look like you "prevented" diabetes if you consider people who dropped their blood sugars from say 203 to 185 as "preventing diabetes." But blood sugars of 185 at 2 hours after eating are high enough to kill beta cells and if you look at those people in ten years the picture is very different.
And, in fact, when you look at data from the follow up study of the drug arm of DPPT you see that the "prevention" that they saw vanished as more time passed. It was only very short term.
Three years is far too short a time in which to determine that any treatment prevents diabetes. Gretchen also makes the very valid point which is one that anyone who has spent time in the diabetic community knows: losing weight only "reverses" diabetes in 5-10% of those who have it. There is very little evidence that diet and exercise will prevent diabetes in people who have the genes that are associated with it over the decades that it takes to develop diabetes.
I've been at the same gatherings of people with diabetes that Gretchen mentions. No one was obese. We were all diabetic, and some of us were using insulin. Diabetes is far more complex than can be explained in a single comment, but your post does not live up to your usual standard of careful reviewing of the literature to go beyond "what everyone believes' to "what has actually been proven by well-constructed research."
Re "multiple lines of evidence suggest that this is because excess body fat causes insulin resistance" I just want to offer an interesting (IMO) anecdote.
Not sure if you would use fasting insulin as a measure of insulin resistance, but at the start of my weight loss efforts, mine was 24. After losing some weight, I retested and it was 12, and thought I'd add exercise. Next re-test, it was 14, and I decided, per your "it's a measure of fat mass" that it wouldn't come down until I'd lost the additional weight.
This spring, I did 60 days of what I was calling my Mat Lalonde-inspired diet of meat, fish, and veggies, which included ~100g of sweet potatoes/day).
Despite still having considerable fat mass, my fasting insulin after this experiment was 4.
It's just an n=1, but it seems interesting in the context of Staffan Lindeberg's diabetes study which showed improved glucose tolerance when dietary source of carbs wasn't grains or dairy.
That's really interesting Beth! I've been curious about that as well. Did you blog on your experience at all?
Yes, quite a bit. Here's the last post where I talk about the blood work.
BTW, just a couple of additional points re my comment. I ate 100g of *carbs* in the form of sweet potatoes per day (not 100g of sw potatoes).
Also, my diet prior to this point was also moderately lower in carb. I had been following my version of the Jaminets' Perfect Health Diet to lose weight (my version generally included a 4-Hour-Body-like cheat meal once a week).
When I switched to a lc diet years before diagnosis with T2 I lost 40 pounds of fat, gained 20 lbs of muscle. A few years later retinopathy persuaded me I was diabetic, and I continued exercise, went VLC, and against medical advice started metering my BGs. Glucose metabolism went into a steady decline to point of persuading (dumb) internist that I actually was diabetic. I have extensive contemporanious data in my BG/food diaries documenting the inexorable decline. Rob
ps The Diabetic Clinic associated with the U of W was horrible, and I can provide 4-6 hostile statements they made about diabetes, medications, meters etc which were simply false.
pps My wife and I are great fans of U of WA hospital.
Hi Kindke,
I like that first reference, I'll have to take a closer look. Regarding the second one, the problem is that ATGL has a major effect on brain lipid metabolism, so the phenotype may be the effect of several interacting factors including some coming from the CNS (which has a strong impact on insulin and glucose metabolism). Personally I don't think it offers strong evidence against the energy overload hypothesis.
Here are a few papers that I find informative re: the idea that lipid overload contributes to insulin resistance in obese humans.
www.ncbi.nlm.nih.gov/pubmed/10480616
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC370462/
http://www.ncbi.nlm.nih.gov/pubmed/1885781
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC293539/
Hi Beth,
That is a remarkable change to be sure. However, I will caution that it's not clear that reduced fasting insulin reflects increased insulin sensitivity in cases like that (although I suspect that in your case it did at least somewhat).
For example, low-carbohydrate diets tend to reduce fasting insulin and so the HOMA score (estimated IR) suggests improved insulin sensitivity. Yet when you directly measure insulin sensitivity by the gold standard euglycemic-hyperinsulinemic clamp technique, it typically hasn't changed or has even worsened. For example, in this study a VLC diet reduced fasting insulin relative to HC, but decreased insulin sensitivity during a euglycemic-hyperinsulinemic clamp (http://www.ajcn.org/content/73/3/554.long).
The point is that fasting insulin is good for estimating insulin sensitivity between people eating a similar diet, but not necessarily good for estimating changes in the same person on different diets. But as I said, I suspect that your insulin sensitivity did improve at least somewhat because you were eating a high-quality diet not too low in carbohydrate.
Can you have type 2 without insulin resistance (ie with only impaired beta cell function from elevated FFA)? I don't understand why IR has to come first.
Thanks!
Hi Stephan
I am somewhat disappointed that your post lacks some of the new data on diet for preventing diabetes.
The WHI-trial that was a randomized long-time trial with a low-fat diet did not prevent diabetes, for those who already had diabetes their glucose control became worse.
http://www.ajcn.org/content/early/2011/05/11/ajcn.110.010843
You mentioned that other diets could prevent diabetes but it hasn’t been tested. There is a trial with different Mediterranean diets comparing low-fat to high fat diet. The high fat diet was associated with the lowest incidence of new diabetes.
http://care.diabetesjournals.org/content/34/1/14.abstract
Hi Dvalinx,
The problem with the WHI intervention is that they didn't lose weight. The trials I cited involved weight loss.
The other trial you cited was interesting, although it was not a comparison between low-fat and high-fat diets. In fact, the total fat content of the three diets were scarcely different. They mostly differed in quality rather than quantity.
http://annals.org/article.aspx?volume=145&issue=1&page=1
The low-fat diet group was just told to eat less fat and sent home. In contrast, the Med diet groups received intensive interventions including meetings, recipes and a long list of dietary guidelines:
"A behavioral intervention promoting the MedDiet was implemented, as described previously (12). In brief, on the basis of the initial assessment of individual scores of adherence using a 14-item questionnaire, dietitians gave personalized dietary advice to participants randomly assigned to both MedDiets, with instructions directed to scale up the score, including, among others, 1) abundant use of olive oil for cooking and dressing, 2) increased consumption of fruit, vegetables, legumes, and fish, 3) reduction in total meat consumption, recommending white meat instead of red or processed meat, 4) preparation of homemade sauce with tomato, garlic, onion, and spices with olive oil to dress vegetables, pasta, rice, and other dishes, 5) avoidance of butter, cream, fast food, sweets, pastries, and sugar-sweetened beverages, and 6) in alcohol drinkers, moderate consumption of red wine."
care.diabetesjournals.org/content/34/1/14.full
It is no surprise that the Med diet groups had a lower diabetes incidence-- despite eating a very similar amount of fat to the low-fat group, diet quality increased considerably.
Hi stew,
Type 2 by definition involves insulin resistance.
The weight loss issue always seems to top the list when it comes to the lifestyle management of diabetes. This was true when I developed gestational diabetes and also now that I have permanent type 2. With no weight to lose (BMI has been 18 all my life), I have found very little information on what to do about diabetes at normal or below normal weight. It's a shame that we can only point a finger at genes at this point and not say anything else about it.
An excellent review of insulin resistance in DM is available (Diabetologia (2010) 53:1270-1287) with an intriguing explanation for why glucose control decreases micro-vascular but not macro-vascular complications. IR occurs in the phosphoninositol-3 kinase pathway (glucose metabolism) but not in the mitogen-activated protein kinase pathway. Much of the debate in this discussion is addressed in the article. “Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: the missing links. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2877338/?tool=pubmed
Here is the abstract:
Insulin resistance is a hallmark of type 2 diabetes mellitus and is associated with a metabolic and cardiovascular cluster of disorders (dyslipidaemia, hypertension, obesity [especially visceral], glucose intolerance, endothelial dysfunction), each of which is an independent risk factor for cardiovascular disease (CVD). Multiple prospective studies have documented an association between insulin resistance and accelerated CVD in patients with type 2 diabetes, as well as in non-diabetic individuals. The molecular causes of insulin resistance, i.e. impaired insulin signalling through the phosphoinositol-3 kinase pathway with intact signalling through the mitogen-activated protein kinase pathway, are responsible for the impairment in insulin-stimulated glucose metabolism and contribute to the accelerated rate of CVD in type 2 diabetes patients. The current epidemic of diabetes is being driven by the obesity epidemic, which represents a state of tissue fat overload. Accumulation of toxic lipid metabolites (fatty acyl CoA, diacylglycerol, ceramide) in muscle, liver, adipocytes, beta cells and arterial tissues contributes to insulin resistance, beta cell dysfunction and accelerated atherosclerosis, respectively, in type 2 diabetes. Treatment with thiazolidinediones mobilises fat out of tissues, leading to enhanced insulin sensitivity, improved beta cell function and decreased atherogenesis. Insulin resistance and lipotoxicity represent the missing links (beyond the classical cardiovascular risk factors) that help explain the accelerated rate of CVD in type 2 diabetic patients.
Anna, Some docs assume that anyone who gets diabetes as an adult is type 2, which is insulin resistance by definition. You might be LADA or MODY. Unless your doc has looked into these ask for a C-peptide test (to see how much insulin you're producing) and a GAD test (to see if you're producing antibodies that suggest type 1). There are tests for MODY, but they're very expensive. Jenny has lots of information about MODY: http://www.phlaunt.com/diabetes/14047009.php.
Obesity may be CORRELATED with insulin resistance but is it the CAUSE? Which came first, the chicken or the egg?
How do you explain insulin resistance in a person who is NOT obese?
I was highly insulin resistant when I was of normal body weight, as indicated by blood testing including C-peptide. Symptom-wise I had severe PCOS and hypoglycemia. These were present from the time I began menses at 13. The weight came much, much later, in my late thirties.
I never ovulated without fertility drugs ever UNTIL I drastically reduced carbs in my diet. I ovulated spontaneously almost immediately (within 30 days) after cutting carbs and before any appreciable weight loss occurred. My second child was easily conceived on a low carb regimen, but to conceive my first child we needed years of fertility drugs and IVF rounds. I ate a "normal healthy" diet then.
My daughter is exactly in the middle of the growth chart for her age height and weight--50th percentile. She is just beginning her menses, and symptoms are indicating insulin resistance in her too. And she has just been diagnosed with PCOS--based on blood tests. There's no weight to lose here, yet she is insulin resistant. This does not fit your theory.
Gretchen, thanks for your remark. I was tested for GAD (none) and C-peptide (1.98, within normal range). So I am not LADA or type 1. Maybe MODY - but my endo has to see whether she can arrange for me to be tested, as it is very expensive and not always covered by insurance. In any case - what will change for me in terms of treatment options and outcome if I receive a positive MODY diagnosis?
There's more than one cause of insulin resistance-- that does not undermine the fact that excess fat mass is the most common.
Hi Gunther,
Thanks for the video link. I have to persue it later, since I cannot see clips from where I am at the moment. Have you read Ian Spreadbury's paper? I'm very curious what you and others think of his theory. It would explain almost... everything! Even anorexia 'nervosa', if you ask me (AN could just be a 'paradoxical' phenotype of the same grain induced endotoxaemia, where it results in anorexia and lipodistrophy). I'm a bit surprised that this 'sources of acellular carbohydrate cause LPS-intoxication causes hyperphagia and all the features of metabolic syndrome' is hardly discussed in the relevant places. Just saw that Emily Deans braught it up though.
People tend to not follow links, so I hope Stephan doesn't mind if paste the abstract:
Ian Spreadbury
Gastrointestinal Diseases Research Unit, Queen's University, Kingston, Ontario, Canada
Abstract: A novel hypothesis of obesity is suggested by consideration of diet-related inflammation and evolutionary medicine. The obese homeostatically guard their elevated weight. In rodent models of high-fat diet-induced obesity, leptin resistance is seen initially at vagal afferents, blunting the actions of satiety mediators, then centrally, with gastrointestinal bacterial-triggered SOCS3 signaling implicated. In humans, dietary fat and fructose elevate systemic lipopolysaccharide, while dietary glucose also strongly activates SOCS3 signaling. Crucially however, in humans, low-carbohydrate diets spontaneously decrease weight in a way that low-fat diets do not. Furthermore, nutrition transition patterns and the health of those still eating diverse ancestral diets with abundant food suggest that neither glycemic index, altered fat, nor carbohydrate intake can be intrinsic causes of obesity, and that human energy homeostasis functions well without Westernized foods containing flours, sugar, and refined fats. Due to being made up of cells, virtually all "ancestral foods" have markedly lower carbohydrate densities than flour- and sugar-containing foods, a property quite independent of glycemic index. Thus the "forgotten organ" of the gastrointestinal microbiota is a prime candidate to be influenced by evolutionarily unprecedented postprandial luminal carbohydrate concentrations. The present hypothesis suggests that in parallel with the bacterial effects of sugars on dental and periodontal health, acellular flours, sugars, and processed foods produce an inflammatory microbiota via the upper gastrointestinal tract, with fat able to effect a "double hit" by increasing systemic absorption of lipopolysaccharide. This model is consistent with a broad spectrum of reported dietary phenomena. A diet of grain-free whole foods with carbohydrate from cellular tubers, leaves, and fruits may produce a gastrointestinal microbiota consistent with our evolutionary condition, potentially explaining the exceptional macronutrient-independent metabolic health of non-Westernized populations, and the apparent efficacy of the modern "Paleolithic" diet on satiety and metabolism.
Gunter & Melchior,
SpreadBerry's (sorry, Spreadbury's) Cellular paper is very interesting.
For me, it adds another (plausible) mechanism to Lindeberg's version of Gardening Paleo rather than Cordain's rampant Grokking.
I am a macro agnostic. I've been a Hearty Peasant food eater for decades, and include lots of KerryGold and Irish potatoes in that - of course, at a meal where I'm hungry and eat to belly satiety.
"I eat when I'm hungry,
And drink when I'm dry,
And if moonshine don't kill me,
I'll live till I die."
http://www.youtube.com/watch?v=El3a-1bSIZM
I do have the following observation about the paper:
In Table 1, the authors give a zero status to the acellular content of Masai 1971 milk content, and + to the Turkana 1980 mostly milk content. Perhaps it's because milk has a CHO density of about 5 gms/100 gms.
Slainte
LeonRover, I would guess Guiness has exactly the right carbohydrate density too ;-). A pseudo cellular carbohydrate, and nicely in line with the drunken monkey theory as well.
Lindeberg's macronutrient agnostic model is getting too little attention, yet it performs best in the small trials that have been done. I wonder if the supposed 'paleo faillures' ("Well, we were eating wonderbread in the sixties too, so it can't be that bad") have really tried it.
'..Cellular energy overload causes insulin resistance, and this occurs when fat tissue expands to the point where it no longer efficiently traps fatty acids, exposing tissues throughout the body to excess energy. In addition, enlarged fat depots tend to become inflamed, and inflammation contributes to insulin resistance. ..'
Can't argue with that. However, like Kindke I find the term energy overload problematic. I expect you're using it as shorthand for a pathway that looks like this
fatty acids --> ROS --> endoplasmic reticulum stress --> unfolded protein response --> inflammation.
But normal levels of fatty acids don't do this. I think the problem might be the pattern of fatty acid delivery to cells. We know they oscillate in the blood, and they might have to do this to prevent 'energy overload'. We know insulin has to oscillate to prevent insulin resistance.
So the 'expanded fat tissue' which 'no longer efficiently traps fatty acids' might mean dysfunctional adipocytes which don't oscillate properly.
Melchior, actually the clip about bacteremia I wanted to paste was this. The first one was about bacteremia from your OWN gut bacteria crossing the BBB, but this one is about bodywide infection from meats we ingest:
http://www.youtube.com/watch?v=9Pnan0ETlVE&feature=plcp
LeonRover,
"Macro Agnostic"! You made my day.
I'm holding out for gut permeability>bacteria>infection>inflammation to be revealed as the major cause of obesity. It's just too weird how poultry workers have such a significantly higher chance of getting weird cancers, obesity and neurological disease.
Check these out, a virus from chickens that makes them obese, as well as those who eat them, and even the workers who kill them:
http://www.youtube.com/watch?v=9lHwRhkkYQY&feature=plcp
and
http://www.youtube.com/watch?v=Zab6_WmyipQ&feature=plcp
Hi, gunther
I lean towards an agnostic view of diet composition as well. I think it is the responsible thing to do. Dr. Jeffrey Friedman is also an agnostic. He simply is uncertain, unsure and does not known yet. I applaud him for being an honest scientist.
I'm center of the road. It just turns out that way as far as my own diet. I try to determine what I might need. I need adequate carbohydrates for my walks interspersed with a few sprints.
Take care,
Raz
Or maybe:
gut permeability>bacteria>infection>inflammation of hypothalamus(???)>obesity
Just thinking out loud.
Gretchen said...
"Anna, Some docs assume that anyone who gets diabetes as an adult is type 2, which is insulin resistance by definition."
That's disappointing that they would do that. My cousin developed Type 1 at age 30 and has to take insulin injections. The American Diabetes Association even created a new diabetes category for adult-onset Type 1 diabetes: Type 1B.
I don't know for sure whether it's related or not, but he developed Type 1B a few years after switching to a grain-rich vegetarian diet that his wife convinced him to adopt. He discovered that he was highly sensitive to wheat. Both their children developed Type 1 at an early age while they were all eating a grain-rich plant-based diet. He read Dr. Bernstein's Diabetes Solution book after I told him about it and he reported that they are doing much better health-wise.
Stephen (or anyone who's been weighing in in the comments): are you aware of any efforts integrate the results of research conducted with respect to the role of fat metabolism in the etiology of diabetes with the results of research conducted with respect to role of methylglyoxal produced as the result of glucose metabolism? (See, for example, "Chronic methylglyoxal infusion by minipump causes pancreatic beta-cell dysfunction and induces type 2 diabetes in Sprague-Dawley rats," available at http://www.ncbi.nlm.nih.gov/pubmed/21300844, and referring to "high carbohydrate-induced type 2 diabetes" using syntax that would indicate the existence of more than one recognized etiology for type 2, at least one of which is involves the high consumption of carbohydrate.) It is the research into the glucose metabolism-overproduction of methylglyoxal--bad news for beta cells and other metabolic processes chain that is leading some folks into extolling the virtues of nutritional ketosis as a means of forestalling further damage.
Sorry--misspelled your name, Stephan.
@PaleoPhil: Type 1B is type 1 without antibodies, called idiopathic type 1, ketosis-prone diabetes, or Flatbush diabetes.
There's a Web site devoted to it:
http://ketosisprone.blogspot.com/
Adult-onset diabetes is LADA, latent autoimmune diabetes of adults.
Stephan, Yes, there are many causes of IR. And some of us think that progress would come faster if scientists and popularizers focussed on the commonalities instead of constantly talking about "the obesity epidemic" and publishing photos of headless fat people.
Some conditions that cause IR include obesity, starvation, third-trimester pregnancy, stress, puberty, surgery, burns, other illness, hibernation, steroid drugs, bedrest, and high blood glucose levels.
Clearly, it's not simple. And obesity, like IR, also has many causes.
Healthy articles
Ian Spreadbury abstract link very interesting reading, thanks.
Gretchen said... "Type 1B is type 1 without antibodies, called idiopathic type 1, ketosis-prone diabetes, or Flatbush diabetes."
Yes, I knew it was also called idiopathic (of unknown cause), though I hadn't heard of the Flatbush term, thanks (and I see that Flatbush reportedly can also be a variant of Type 2, as well as Type 1: http://articles.nydailynews.com/1999-11-22/entertainment/18111891_1_dka-insulin-blood-sugar, so there is apparently overlap between Types 1 and 2, interestingly). What I meant was that idiopathic type 1 is sufficiently common and well known to get it's own subcategory of Type 1B http://www.ncbi.nlm.nih.gov/pubmed/15111529, so it's disappointing that some physicians are apparently not being educated about it and the overall complexity of diabetes and might miss that an adult who doesn't fit the T2DM mold is developing another form of adult-onset diabetes like T1bDM and go undiagnosed for some time.
Thanks for sharing the MODY and LADA terms, Gretchen. After reading about them and other Type 1 subtypes, I'm wondering whether my cousin has been tested to determine which one he really has. He might not care, as I haven't noticed any reported differences in clinical treatment based on Type 1 subtype.
The more I learn about various subcategories of diabetes and about blood sugar problems in general, the more complexity I find. I came across this that I thought was a good summation: "I like the idea that diabetes is a spectrum of disease, with autoimmune type 1 in children on one end, and metabolic type 2 in adulthood on the other end." - Sarah Howard, National Coordinator, The Collaborative on Health and the Environment's Diabetes-Obesity Spectrum Working Group, http://www.diabetesandenvironment.org/home/conditions/diabetes
I found this study today, it talks about something called lon protease which "degrades oxidatively damaged proteins in mitochondrial matrix"
Lowering lon protease apparently induces IR, I guess this fits in with the theory that insulin resistance is a cellular antioxdiant defense mechanism.
Im just posting this to further confirm what everyone knows, that is that IR is indeed very complicated.
However to say that increased fat mass causes IR is akin to saying that increases in the diameter of cellular lipid droplets causes IR..... now is that true?
Of course, if you are overweight your doctor is much more likely to test you for IR and DM2, because he thinks this association is real. So there will be more early diagnoses in the overweight. And fewer in those who look normal; their symptoms will be put down to psychosomatic causes, they'll be prescribed mood drugs that make them fat, and then they can have a proper "obese DM2" diagnosis...
In any case, there is probably a bias towards looking for type 2 diabetes in overweight individuals.
Ketogenic diet (low carb) reverses renal failure in mice
Abstract
Intensive insulin therapy and protein restriction delay the development of nephropathy in a variety of conditions, but few interventions are known to reverse nephropathy. Having recently observed that the ketone 3-beta-hydroxybutyric acid (3-OHB) reduces molecular responses to glucose, we hypothesized that a ketogenic diet, which produces prolonged elevation of 3-OHB, may reverse pathological processes caused by diabetes. To address this hypothesis, we assessed if prolonged maintenance on a ketogenic diet would reverse nephropathy produced by diabetes. In mouse models for both Type 1 (Akita) and Type 2 (db/db) diabetes, diabetic nephropathy (as indicated by albuminuria) was allowed to develop, then half the mice were switched to a ketogenic diet. After 8 weeks on the diet, mice were sacrificed to assess gene expression and histology. Diabetic nephropathy, as indicated by albumin/creatinine ratios as well as expression of stress-induced genes, was completely reversed by 2 months maintenance on a ketogenic diet. However, histological evidence of nephropathy was only partly reversed. These studies demonstrate that diabetic nephropathy can be reversed by a relatively simple dietary intervention. Whether reduced glucose metabolism mediates the protective effects of the ketogenic diet remains to be determined.
PLoS One. 2011 Apr 20;6(4):e18604.
@Kindke
Have another look at that paper you posted showing that mice on a high-fat diet whose fat mass was held constant did not develop insulin resistance. It seems to show it's the increased fat mass rather than the high-fat diet that's the problem, right?
Well, it might not show that. The fat-mass-clamped mice were fed once a day, unlike the others who were fed ad lib. I don't see how else the experiment could have been done, but it means the clamped mice had the benefit of fasting-induced autophagy.
Stephan,
Any thoughts on Ray Peat's view that excess stress hormones cause diabetes (and the subsequent hight sugar - especially fructose - diet for diabetes)?
This posting suggests insulin resistance leads to larger production of insulin from the beta cells. This is followed by beta cell exhaustion (in which eventually the beta cells can no longer produce enough insulin), and then to diabetes?
What is the evidence for this? Or is it merely presumed that the decline in beta cell insulin production is due to "exhaustion"?
Assuming it is so, surely the implication is to limit total insulin production so that the beta cells last longer. If you were told you would have only one car during your lifetime (and it could not have major repairs) you would minimize the miles driven. Likewise, it would seem that trying to limit the load on the beta cells would be prudent. If this is right, this would seem to be a strong argument for eating more fats and fewer carbohydrates, as well as for eating lower glycemic index foods in general.
Yet most discussions of diet seem to focus on merely which diets reduce or increase insulin resistance, rather than on postponing the transition from only insulin resistance to diabetes.
Am I missing something?
ProfessorEd,
Beta cells are not like cars. They repair themselves. The problem is not carbohydrate per se, it's refined carbs that do not have the nutrients needed for beta cell repair.
Here's a paper about beta cell repair.
'Type 2 diabetes mellitus is characterized by insulin resistance and failure of pancreatic beta-cells producing insulin. Mitochondrial dysfunction may play a role in both processes of diabetes. Autophagy maintains cellular homeostasis through degradation and recycling of organelles such as mitochondria. As dysfunctional mitochondria are the main organelles removed by autophagy, we studied the role of autophagy in diabetes using mice with beta-cell-specific deletion of the Atg7 gene. Atg7-mutant mice showed reduction in beta-cell mass and pancreatic insulin content. Electron microscopy showed swollen mitochondria and other ultrastructural changes in autophagy-deficient beta-cells. Insulin secretory function ex vivo was also impaired. As a result, Atg7-mutant mice showed hypoinsulinemia and hyperglycemia. These results suggest that autophagy is necessary to maintain structure, mass, and function of beta-cells. Besides its effect on beta-cells, autophagy may affect insulin sensitivity because mitochondrial dysfunction has been implicated in insulin resistance and autophagy is involved in the maintenance of the organelles. Furthermore, since aging is associated with impaired glucose tolerance, decline of autophagic activity may be involved in age-associated reduction of glucose tolerance.'
http://www.ncbi.nlm.nih.gov/pubmed/20649543
ceWHY PURE SANTE BARLEY IS GOOD FOR DIABETES
www.puresantebarley.blogspot.com
Barley is an excellent whole grain choice because it has a high concentration of dietary fiber, including beta-glucan soluble fiber. Studies have confirmed that beta-glucan soluble fiber is effective in promoting healthy blood sugar, reducing cholesterol, promoting healthy blood pressure and helping control weight, all conditions associated with diabetes.
“Pure Sante Barley has become a rising star as a recommended food choice for those concerned about type 2 diabetes or pre-diabetes,” says Mary Palmer Sullivan, Executive Director, National Barley Foods Council. “The grain contains essential vitamins and minerals and is an excellent source of dietary fiber, particularly beta-glucan soluble fiber.”
Findings from clinical trials reported in Nutrition Research and the Journal of the American College of Nutrition showed that people who ate foods containing barley experienced significant reductions in glucose and insulin responses compared to responses after eating similar products containing whole wheat and corn. Another study published in the Diabetes Research and Clinical Practice Journal reported a 30-percent decrease in HbA1c (average blood glucose level) in people with type 2 diabetes who ate a healthy diet including pearl barley that supplied 18 grams of soluble fiber per day.
Barley is available in whole grain or pearled forms including flakes, kernels, flour and grits. For more information about barley and diabetes, additional health benefits, and testimonials
www.puresantebarley.blogspot.com
FOR ORDERS YOU MAY CONTACT ME
TNT: +639107021656
TM: +639263520154
Email: puresantebarley@gmail.com
Skype: puresantebarley
VERGEL ALDOUS JAVA
Associate Director
"Some conditions that cause IR include obesity, starvation, third-trimester pregnancy, stress, puberty, surgery, burns, other illness, hibernation, steroid drugs, bedrest, and high blood glucose levels."
And gluten intolerance/celiac and create a starvation like situation by way of malabsorption.
hey dude this is really good blog to know some interesting news.I recently Visit your Blog and read about this topic.so interesting topics.i am go to bookmark on this page and i am also tell my friends to visit your blog and get some information.i'll daily visit your blog and give some new blogs.If You get Some information About Wight loss just visit What is the paleo diet
@ Dr. Bob -
While the study you posted has seemingly interesting conclusions on the surface, we must recognize that due to it's short duration of a mere 8 weeks that it doesn't take into account the 'bell-curve effect' so many people experience on an overly carb restricted diet. While this approach may make for a great 'jump-start' for someone at serious risk, it's ability to be a sustainable long-term approach is suspect. I too personally experienced benefits of severe carb restriction - short term - then found those benefits to disappear and negative side effects emerge as a Type I diabetic. My blood sugar control is much better when eating an amount and type of carbohydrates congruent with the amount and intensity of my physical activity.
@ ProfessorEd,
All ingested foods cause insulin production. We must be careful not to make overly generalized statements regarding the type and amount of nutrients to ingest. each case must be examined individually. One must also first distinguish between refined/processed carbs and those that are not. 1 pound of broccoli is surely different than 1 pound of bagels, which is yet again different from 1 pound of potatoes.
Moving forward the individuals amount and intensity of level of their activity must be acknowledge and then wisely paired with a matching type and amount of carbohydrate. This is the problem with those professionals who reccomend certain percentages of diets coming from this nutrient and that nutrient. One who resistance trais requires more protein than one who does not. One who partakes in very high intensity or very long-term duration activities require more carbohydrates than one who sits at a desk 40-60 hours a week.
All my four grandparents died of diabetes and heart related problems. We also have many relatives with this disease. One of them died with an amputated leg. Now my mother has type 2 diabetes and mild heart complications. This makes me wonder if diabetes is a hereditary disease in my family lineage. If it's hereditary, could my siblings and i be in danger of being sick with diabetes? Will good nutrition guarantee our safety? I am so scared of this disease.
Thanks for this helpful reminder. I myself is now at risk of having type 2 diabetes mellitus so I'm getting as much information as I can about this matter.
Post a Comment